Defining the future of digital health experiences
As the leader in patient engagement, we have helped healthcare organizations differentiate themselves in meaningful and measurable ways for more than 20 years. We offer a uniquely personal patient and family experience based upon a very straightforward operating standard: An informed, involved patient and family leads to better outcomes.
With the largest portfolio of patient engagement solutions in the market, Get Well’s flexible approach to patient engagement enables organizations to tailor the method and amount of communication to each individual patient. This ensures patients feel connected, prepared, and informed at every step of their health journey.
What sets us apart
Today, our comprehensive digital patient engagement offerings provide a seamless experience for every patient and their family, personalized to their healthcare needs and reaching them across a full episode of care, as well as in between episodes. Get Well leaves no patient behind, allowing you to reach a wider population while elevating outcomes and reducing unnecessary costs. With our current portfolio of engagement solutions, we enable organizations to provide patients with a branded, consistent, and unified digital experience that engages patients wherever they are. With Get Well, organizations can provide:
- Step-by-step care journeys that drive high engagement levels and adherence to treatment plans
- Augmented patient care that saves clinician time with automated tasks and escalation of patients for timely intervention and triage
- Modern digital tools that are available before, during, and after a hospital stay
- Virtual care support offered via videoconferencing, AI-driven real-time SMS, and asynchronous messaging
- Longitudinal engagement and activation that brings patients back in network for new episodes, including personalized outreach at scale that uses AI-powered text and services
- Cross-continuum communication that enables your care teams to coordinate efforts and elevate outcomes
For the patient
- Engage with a connected and continuous digital experience
- Receive constant support that organizes and contextualizes tasks so you can stay on track with your care plan
For the care team
- Scale the reach of care teams
- Manage by exception and intervene before costs and complications arise
- Increase patient care plan adherence
For the hospital
- Offer a consistent, consumer-grade digital experience for patients
- Better control total cost and quality of care
- Grow share-of-wallet by keeping patients in-network for new episodes of care
Outstanding patient engagement across care settings
Get Well offers consumer-grade, patient-centric solutions that are designed to be easy to access and use and truly helpful to the patient. Patients receive the right information at the right time wherever they are and can choose to access that information in the way that is most convenient for them. While patient portals commonly report low patient adoption rates, Get Well’s solutions consistently deliver.
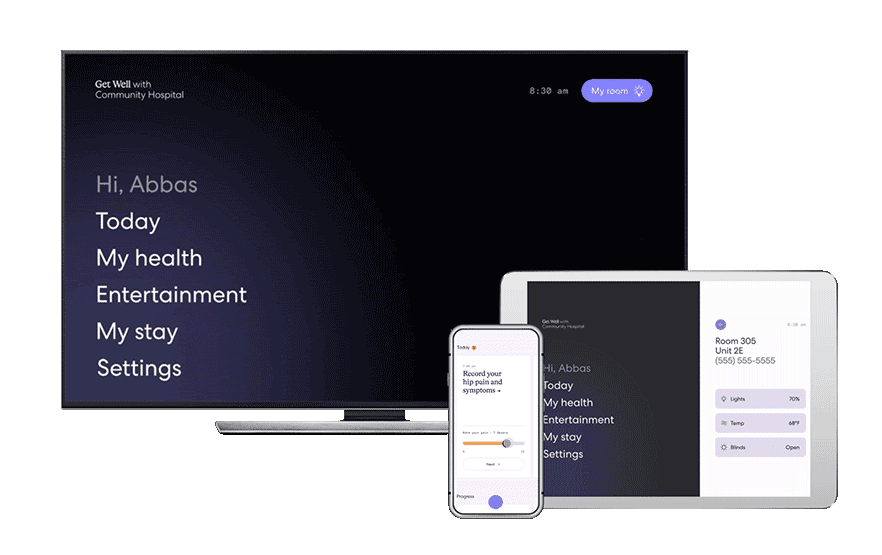
Experience the difference
We’ve brought the Get Well experience to the patient’s fingertips. By providing access to Get Well content and functionality on personal smartphones and tablets, patients can use a device with which they’re familiar to engage in their care. Allowing patients to use the device of their choice boosts engagement and utilization and supports a consistent system-wide experience.
Industry-leading library of longitudinal digital care plans
Get Well understands you need content targeted to the unique needs of your patients. With Get Well, organizations do not have to build their own content from scratch.
Our library includes more than 230 evidence-based episodic digital care plans designed for patients undergoing procedures or dealing with chronic illness across both inpatient and ambulatory settings. Each care plan consists of education, reminders, assessments, and tasks broken down into bite-sized chunks and delivered to the patient automatically over a schedule of weeks or months.
Get Well’s care plans:
- Step-by-step care journeys that drive high engagement levels and adherence to treatment plans
- Augmented patient care that saves clinician time with automated tasks and escalation of patients for timely intervention and triage
- Modern digital tools that are available before, during, and after a hospital stay
Seamless integration into existing clinical and EHR workflows
Get Well recognizes the importance of allowing clinicians and patients to directly access our solutions from within the EHR and patient portal. That’s why we’re embedding our capabilities directly into these core platforms to provide clinicians with a digital framework that streamlines workflows and improves communication and care coordination.
We’re also unifying the patient experience by embedding our solutions within EHR consumer access points. This means that patients can access Get Well capabilities within the EHR portal experiences with which they’re already familiar — meaning no extra logins to remember or websites to visit. It’s one more way we help to engage patients and families by meeting them on their terms.
Driving value beyond technology
Get Well has an experienced client success team dedicated to:
- Managing and simplifying the adoption process
- Tailoring technology to meet unique clinical and operational workflow needs
- Tracking and driving utilization and outcomes
- Increasing overall speed to value
We have prioritized and invested in executive-level talent who serve as strategic thought partners to our clients’ executive teams. This ensures that Get Well technology and services are aligned with key client initiatives and outcomes and will drive value.
The Get Well experience
At home
Procedure prep
- 230+ personalized care plans
- Virtual check-ins
- Pre-admission optimization
- Seamless surgical preparation
- Two-way communication with care team
In the hospital
Admission and discharge
- Guided education care plans
- Real-time patient satisfaction feedback
- Digital rounding
- Automated service request triage
- Videoconferencing
- Patient meal ordering
- Environmental controls
- Entertainment
At home
Successful recovery
- Remotely monitor patients/daily patient monitoring
- Secure messaging
- PROMs collection
- Physician/facility reviews and rating
Virtual care
Intelligent patient activation
- Drive new volume by re-engaging dormant populations
- Activate vulnerable populations
- Enroll, retain, and coordinate care for health plan members
- Enhance patient profiles through every interaction
